

Studies have shown that using tPA within 3 hours of stroke onset raises the chances for good outcomes in some patients who suffer one of these events, but this treatment is often underused. Although more than 11% of patients with stroke are eligible to receive tPA, studies show that 2% or less receive these important thrombolytics. Eliminating delays in the recognition and response to signs and symptoms of stroke could increase the proportion of tPA-eligible patients to as high as 24%.
Designated stroke centers have improved the delivery of tPA, but less than one-quarter of patients in the United States live within 30 minutes of one of these centers. “The importance of early treatment for stroke cannot be overstated,” says Phillip A. Scott, MD. “Because of the short treatment window in which tPA can be given, many patients seek treatment at local community hospitals.” Unfortunately, neurologists are frequently unavailable for acute stroke care in community EDs. Furthermore, ED physicians often are hesitant to use thrombolytics due to time and resource issues or lack of experience with tPA.
The INSTINCT Trial
Few randomized controlled trials have tested practical interventions to increase tPA delivery for stroke patients in community hospitals. Identifying successful interventions could improve stroke care and serve as a model to enhance the adoption of other high-risk treatments. In an effort to increase tPA use in community hospital settings, the Increasing Stroke Treatment through Interventional Change Tactics (INSTINCT) trial was initiated in Michigan.
The goal of INSTINCT was to assess the ability of a multilevel, barrier assessment-interactive educational intervention to increase tPA use in community hospitals, explains Dr. Scott, who was lead author of the study. The authors also wanted to identify and explore local barriers to tPA use in patients with stroke. Researchers involved in INSTINCT collected baseline data on stroke treatment at participating hospitals with at least 100 stroke discharges per year that were not classified as academic comprehensive stroke centers. They then randomized some locations to receive an intervention consisting of CME classes, workshops, and other support, including 24-hour phone consultation availability.
Key Findings: tPA Safe in Community Hospital Setting
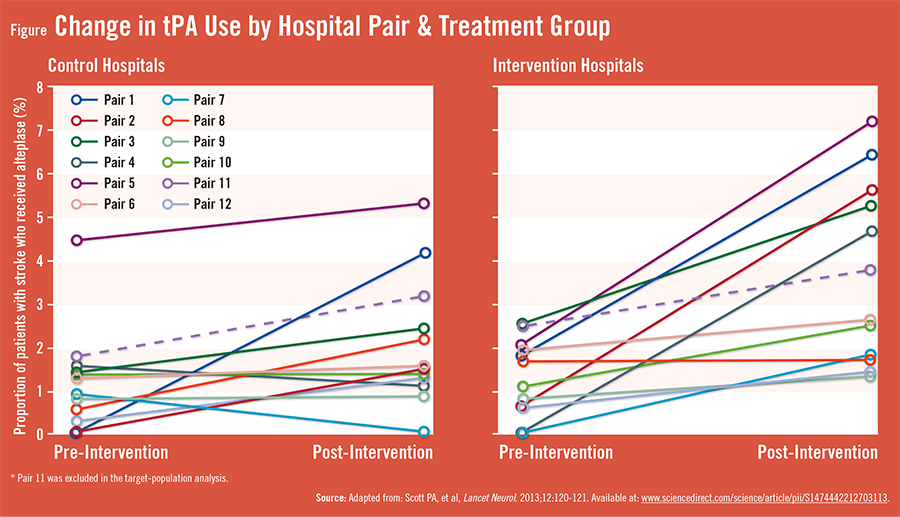
According to findings published in Lancet Neurology, tPA could be used safely and appropriately in the community hospital setting without increasing risks of dangerous bleeding. Data showed that tPA use increased significantly in the target population of community hospitals that were randomly chosen to get the intervention (Figure) compared with the control group. “We essentially saw a doubling of tPA usage by using standard technologies for education and support that was achieved safely,” Dr. Scott says. Notably, a smaller increase in safe and appropriate use of tPA was observed in the hospitals that did not receive the intervention.
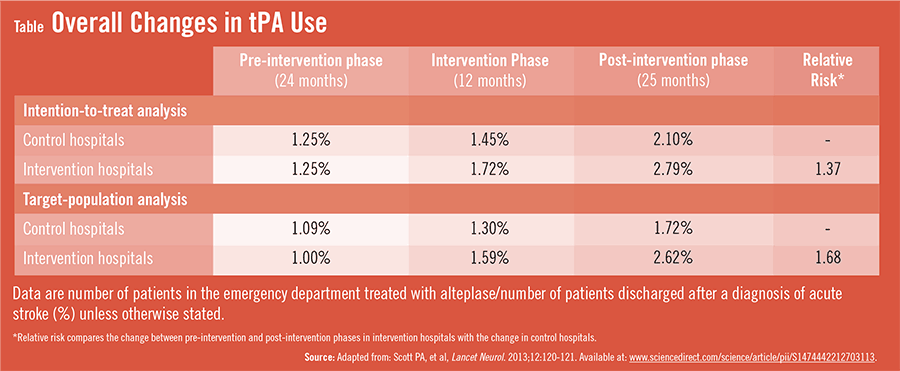
In the target population (22 total hospitals), the percentage of patients treated with tPA increased between the pre- and post-intervention phases, rising from 1.00% to 2.62% in the intervention group, and from 1.09% to 1.72% in the control group. The difference between the change in the intervention group (a 1.62% absolute increase) and the change in the control group (0.63%) was 0.99%, which equated to a 104% difference in relative increase in tPA use (Table). “Some hospitals even surpassed national targets for tPA use that larger stroke centers don’t always reach,” adds Dr. Scott.
Important Implications on Effective Stroke Treatment
The findings demonstrate that hospitals and EDs can translate the knowledge of effective stroke treatment into a community setting with relatively low-cost and low-tech interventions, says Dr. Scott. “Awareness programs and initiatives have boosted tPA use, but more work is still needed to expand public access to tPA. The improvements observed at community hospitals receiving our intervention were statistically significant, but they were modest on average.”
INSTINCT offers key insights into the challenges faced by hospitals to create pragmatic interventions to improve knowledge on how to safely increase rates of tPA use. “It’s clear that many community hospitals can evaluate and treat enough emergency stroke patients to keep their teams’ treatment skills sharp,” Dr. Scott says. “The smaller size of some of these hospitals allows for shorter lines of communication between the ED, neurologists, radiologists, and others to safely diagnosis and care for stroke. Importantly, INSTINCT lays the groundwork for future strategies that should be explored to develop evidence-based interventions that have the potential to improve patient access to tPA following stroke. Finding these additional strategies are critical to enhancing outcomes in acute stroke treatment.”
 admin
admin
{kind=link}
{kind=link}