
“For many years, there have been serious concerns among the medical and lay communities surrounding the use of sunscreen and other sun-protective measures with regard to their potentially detrimental impact on bone health, specifically reduced BMD and and/or increased risk for osteoporotic fracture,” explains Dr. Mohsen Afarideh, MD, MPH. “This is because the ultraviolet (UV) irradiation range of approximately 290-320 nm that is needed to induce effective vitamin D photosynthesis, which is vital for bone homeostasis, is within the photocarcinogenic UV-B spectrum, which is protected by sunscreen use. In addition, there was a lack of studies clarifying this potentially important association.”
Sunscreen Not Linked With Decreased BMD, Fracture
For a paper published in JAMA Dermatology, Dr. Afarideh and colleagues aimed to examine the association of sun-protective behavior with BMD z scores and the incidence of osteoporotic fractures. They conducted a population-based, cross-sectional study with data from adults in the United States who participated in the 2017-2018 cycle of the National Health and Nutrition Examination Survey (NHANES). Researchers included data from 3,418 individuals (average age, 39.5; 1,612 [47.2%] men; and 1,806 [52.9%] women) who completed the NHANES dermatology questionnaire.
“To our knowledge, this is the first study to examine the associations between sun protection, sun sensitivity, BMD, and osteoporotic bone fractures in a population-based setting. We found that regular use of sun-protective behaviors was not linked with reduced BMD or greater risk for osteoporotic fracture,” Dr. Afarideh says. “Sun protection may be associated with a moderate reduction in the rate of osteoporotic fractures, potentially because of risk-averse behaviors. However, the most important takeaway message of our paper is that dermatologists, rheumatologists, and other physicians can point to this large, representative study and reassure patients about the bone-safe profile of sunscreens and other sun-protective behaviors.”
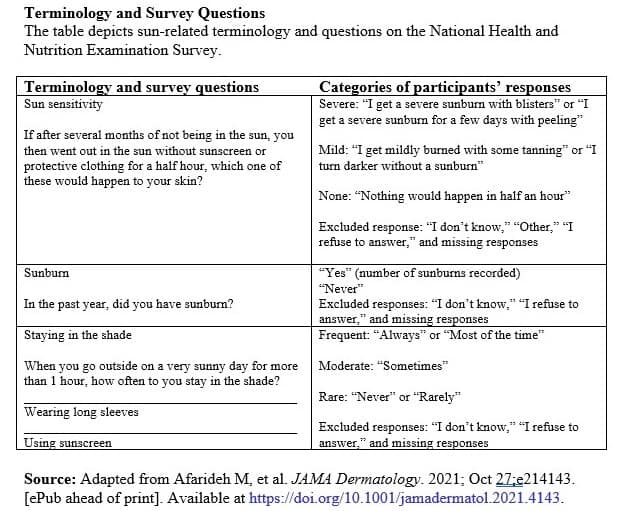
The study team analyzed participants’ responses about their sun sensitivity and sunburn history, as well their sunbathing habits and sunscreen use, Dr. Afarideh says. “However, an important limitation of the study is that the specific type (eg, lotion, moisturizer, spray, etc.) or strength (eg, SPF, UV protection) of sunscreens was not directly asked of participants (Table).”
The rates of frequently staying in the shade, wearing long sleeves, and using sunscreen were 31.6% (95% CI, 27.8% to 35.7%), 11.8% (95% CI, 10.6% to 13.1%), and 26.1% (95% CI, 23.5% to 28.8%), respectively. Individual sun-protective behaviors were not associated with reduced site-specific and total BMD z scores in multivariate models (estimate, −0.23 [95% CI, −0.47 to 0.02]; −0.08 [−0.27 to 0.12]; and −0.10 [−0.32 to 0.13] for frequently staying in the shade, wearing long sleeves, and sunscreen use, respectively). Moderate to frequent staying in the shade was associated with a lower rate of spine fractures in the multivariate model (OR, 0.19 [95% CI, 0.04-0.86]).
More Longitudinal Studies Needed
“According to our findings—and to a growing body of evidence—dermatologists and rheumatologists can continue to safely recommend wearing sunscreens and practicing other sun-protective methods to reduce the risk for major public health concerns, including the melanomatous and non-melanomatous skin cancers, photoaging, and photosensitivity, as well as sun-aggravated dermatoses such as rosacea, lupus erythematosus, and autoimmune bullous disorders,” Dr. Afarideh says.
Given the cross-sectional nature of the study, however, causality could not be established, Dr. Afarideh also notes. “It is still critical to investigate this clinically relevant association through prospective longitudinal studies to establish whether the use of sunscreens (eg, in different SPFs) or other sun-protective measures would impact BMD and/or the risk for osteoporotic fractures,” he says. “In addition, we would like future research to study this association, ideally in the elderly population (aged 65 and older), when the risk for osteoporosis is higher and the risk for traumatic fractures is lower compared with our study population.”
 Martta Kelly
Martta Kelly
{kind=link}