

Requirements for surgical proficiency are generally based on an absolute number of procedures completed, but the pace at which people are trained or become proficient in a procedure tends to be highly individualistic. Skill levels progress at varying speeds. Setting a specific number of procedures for surgical training can lead to surgeons having variable skill levels. As a result, patient safety can be potentially impacted during and after training. Simulation technology has been thought of as a helpful tool to address both patient safety concerns and the varying speeds at which surgical trainees reach proficiency.
A Simulator Is Born
“When endoscopic sinus surgery was popularized in the 1990s, a number of complications were reported because of the proximity to the eyes and brain,” explains Marvin P. Fried, MD, FACS. “These complications included loss of eye muscle motion, vision, and brain fluid leakage. It was a new surgical technique on which surgeons needed training. Lockheed Martin then created a sinus surgery simulator with the purpose of providing a safe environment that looked and felt like human anatomy.”
People who train on the simulator run an endoscope through the nose, and a corresponding image appears on a monitor. Users hold the handle of one of 24 instruments—ranging from needles to forceps—in their other hand. The simulator then measures how long procedures take and whether errors have been made. The technology simulates such things as bleeding when errors are made. Tasks are set to beginner, intermediate, and advanced levels.
Putting Simulation to the Test
Previous studies conducted by Dr. Fried and colleagues at Montefiore Medical Center indicated that the simulator looked and felt like the real thing and allowed trainees, from residents to attending surgeons, to perform in a safe environment. Next, they reported that subjects trained on the simulator made fewer errors and completed procedures quicker than those trained conventionally.
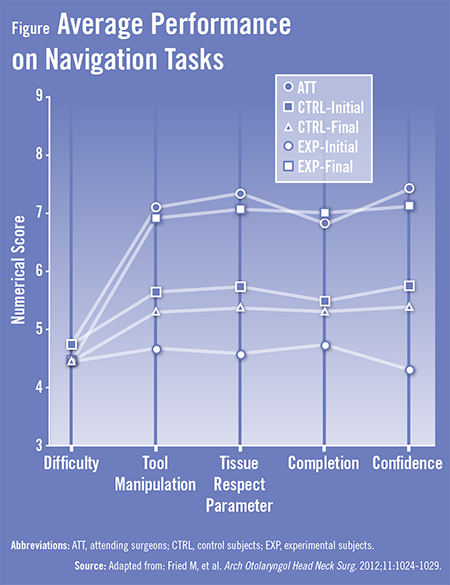
In the Archives of Otolaryngology-Head & Neck Surgery, Dr. Fried and colleagues reported on findings from a study that corroborated previous performance findings with simulators and expanded upon them. For the study, junior residents in otorhinolaryngology were trained using the simulator or conventional methods and then videotaped while performing four tasks as a part of endoscopic sinus surgery (Table). Attending surgeons set the benchmark against which both groups were compared, and a panel of otorhinolaryngologists with expertise in endoscopic sinus surgery judged the anonymous videos based on time to completion of the task, case difficulty, tool manipulation, tissue respect, task completion rate, surgical confidence, and number of errors.
Dr. Fried says that “while all participants were superior when compared with initial procedures, surgeons who were trained on the simulator performed as well, if not better, than those who were trained conventionally. In fact, the performance of those trained on the simulator was indistinguishable from that of attending surgeons in some tasks [Figure].” The simulator allows users to be trained repeatedly in a safe environment without putting patients at risk, adds Dr. Fried. “No patient wants to be told that they’re the first one to be operated on by a particular surgeon. Although there will always be a first patient for surgeons, it’s beneficial to have tools like simulators to help trainees reach proficiency to overcome any concerns about doing a surgery.”
Broader Application
According to Dr. Fried, all surgical specialties could benefit from computer-based simulation. Studies have already established the benefits of simulation for laparoscopic cholecystectomy, for example. “Nearly every surgical specialty is trying to incorporate simulation training into residency programs,” Dr. Fried says. “This type of training needs universal support from practicing physicians. As simulators are developed, hospital leaders should be open to incorporating them into their training programs.”
Dr. Fried adds that Marc Gibber, MD—his co-author on the Archives of Otolaryngology-Head & Neck Surgery article—will continue research that focuses on how simulation fits into surgical education. “With all the data that have accumulated on this topic, it’s clear that surgical simulation is here to stay,” says Dr. Fried. “Using simulators is an important aid in patient safety. As clinicians, we should proactively support efforts to enhance how we train individuals in the future. Simulators provide a safe environment to ensure optimal outcomes for trainees working on their first cases.”
 admin
admin
{kind=link}
{kind=link}