

Interstitial lung disease (ILD) is especially prevalent in anti-tRNA synthetase syndrome (ARS), which classically presents with ILD, arthritis, and mechanic’s hands. However, the frequency of skin, muscle, and lung disease is variable among ARS antibodies, and some patients may have only pulmonary manifestations. Improving the recognition of ARS-ILD is critical to ensuring patients have prompt access to immunosuppressive therapies. “Anti-synthetase syndromes often go underrecognized in patients,” explains Erin M. Wilfong, MD, PhD of Vanderbilt University Medical Center. “Many patients with ARS ask if they would still need oxygen had their disease been recognized earlier. In some cases, the need for oxygen or lung transplant might have been avoided.”
Patients With IIM Less Likely to Meet Clinical CTD Classification
Diagnosing idiopathic inflammatory myopathy (IIM)-ILD continues to be challenging, Dr. Wilfong notes. Guidelines recommend that connective tissue disease (CTD)-related ILD can be ruled out clinically and with basic serologic screening, but they do not recommend comprehensive myositis serologies. Basic serologies are more likely to be negative in IIM when compared to other CTD, but patients with IIM are also less likely to meet clinical CTD classification criteria.
For a study published in Respiratory Medicine, Dr. Wilfong and colleagues compared clinical, radiographic, and serologic features between ARS and IIM and systemic sclerosis. The study group also sought insights into etiologies that can lead to delays in diagnosis and therapy among people with ARS. “We wanted to understand how patients with ARS presented and how we can improve recognition of this disease,” Dr. Wilfong says.
Patients With UIP Pattern CT Scans Are at Increased Risk for Misdiagnosis
Dr. Wilfong and colleagues found that patients with ARS had a high frequency of ILD and more severe pulmonary restriction than other IIM subgroups. In 51.9% of cases, ARS patients had ILD. The severity of forced vital capacity reduction in ARS was comparable to diffuse cutaneous systemic sclerosis (53.2% vs 56.8%, respectively), and greater than dermatomyositis or limited cutaneous systemic sclerosis (66.9% and 71.8%, respectively). Of note, only patients with ARS-ILD had CT reads of usual interstitial pneumonia (UIP). Since UIP pattern CT scans are classically associated with idiopathic pulmonary fibrosis, patients with UIP pattern CT scans are at increased risk for misdiagnosis.
“It’s important to conduct serologic screening for ARS using a myositis panel,” says Dr. Wilfong. “Many providers will send anti-nuclear antibodies, rheumatoid factor, and anti-cyclic citrullinated peptides to screen for CTD-related ILD, but this has poor sensitivity for ARS. If a bead or ELISA-based anti-nuclear antibody test is used—which is common in many commercial labs—the sensitivity drops even further. In addition, our study revealed that patients with ARS can have radiographic UIP. This is important because patients with UIP still need to be screened for CTD.”
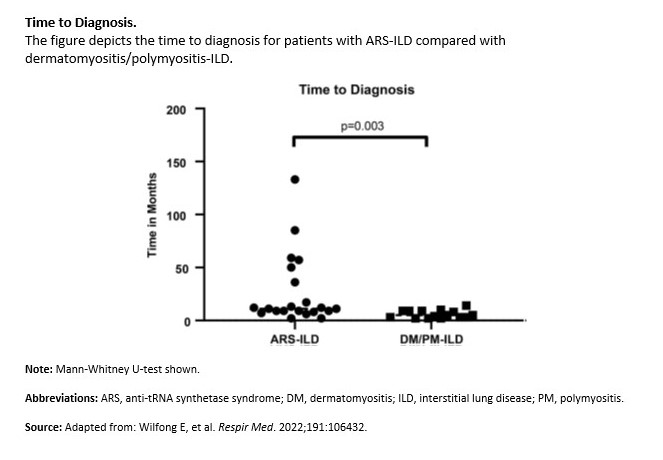
The study also demonstrated that patients with ARS were frequently referred to a tertiary center after seeing a local pulmonologist and/or rheumatologist without receiving a correct diagnosis. Approximately 53.6% of patients with ARS first presented to a tertiary center, because they experienced fewer extrapulmonary manifestations. Another key finding was that patients with ARS-ILD had a two-fold longer median time to diagnosis than those with other myositis-ILD (Figure).
Expert Consultation Critical If There Is Any Suspicion of CTD
Diagnostic delays in ARS have been identified as an independent risk factor for mortality in ARS-ILD. “It’s strongly recommended that providers send immunofluorescent anti-nuclear antibodies and a myositis panel for all patients with a new ILD diagnosis,” says Dr. Wilfong. “Testing for anti-tRNA synthetase antibodies is reliable, but other autoantibodies can have false negatives or false positives. In addition, since we only routinely test for antibodies against 5/20 tRNA synthetases, an expert consultation from a rheumatologist is important if there is any suspicion of CTD.”
The study data highlight the importance of using expanded serologies to help identify IIM-ILD in general and ARS-ILD specifically. “Our study focused on detecting ARS, but we also need to improve recognition of other forms of CTD related ILD,” Dr. Wilfong says. “Over the long term, we need to predict who will respond to specific immunosuppressive agents and who would benefit from upfront anti-fibrotic therapies.”
 Martta Kelly
Martta Kelly
{kind=link}