
According to recent estimates, just less than 3% of Americans have moderate-to-severe valvular heart disease (VHD), a condition that increases in prevalence with age. The disease affects between 4% and 9% of those aged 65 to 75 and 12% to 13% of those aged 75 and older. Many of these patients require surgical or interventional procedures, but even with these treatments, the overall survival rates associated with VHD are lower than expected. The risk of adverse outcomes due to VHD is high because of limited options for restoring normal valve function and because of failures to intervene at the optimal time point in the disease course.
A Welcome Update
In 2008, the American College of Cardiology (ACC) and American Heart Association (AHA) released an updated guideline for diagnosing and managing adult patients with VHD. In 2014, the ACC/AHA updated these guidelines in an effort to facilitate access to concise, relevant information at the point of care when clinical knowledge is needed the most. “In the past 5 years, we have accumulated new evidence and a better understanding of earlier research surrounding VHD,” explains Paul Sorajja, MD, FACC, FAHA, FSCAI, who was a member of the ACC/AHA writing group that developed the most recent guideline update. “Our goal was to provide clinicians with concise, evidence-based recommendations and the supporting documentation to encourage their use.”
Restructured Definitions
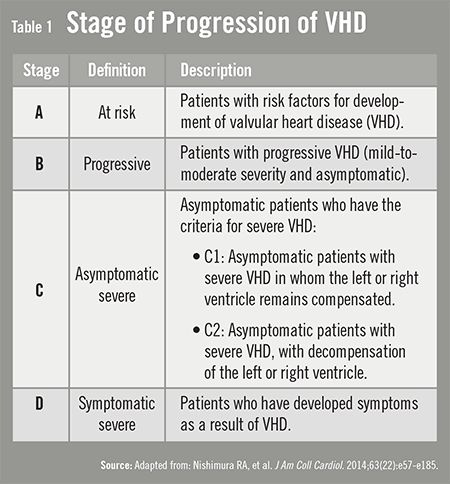
The 2014 guidelines include restructured definitions of VHD severity into four classifications—at risk, progressive, asymptomatic severe, and symptomatic severe (Table 1). “These categories were created to help clinicians determine the optimal timing of interventions,” Dr. Sorajja says. The stages consider the degree of valve narrowing or leakage and the presence of symptoms. They also consider the response of the left and right ventricle to valve lesions and any changes in heart rhythm.
 “Staging of VHD is important because the goal has shifted toward finding at-risk patients earlier so that they can be treated before their condition worsens,” says Dr. Sorajja. “The goal is to avoid cardiac overload early and offer preventive, timely treatments. Doing so may reduce costs and hospitalizations associated with VHD.”
“Staging of VHD is important because the goal has shifted toward finding at-risk patients earlier so that they can be treated before their condition worsens,” says Dr. Sorajja. “The goal is to avoid cardiac overload early and offer preventive, timely treatments. Doing so may reduce costs and hospitalizations associated with VHD.”
Previous guidelines provided limited information on strategies to approach risk assessment. The 2014 update provides assistance with risk assessments for all patients being considered for intervention. The guidelines recommend discussing with patients several important factors when determining the optimal therapy. These include procedure-specific impediments, major organ system compromise, comorbidities, patient frailty, and predicted risk of mortality models, along with more specific risks and benefits.
Transcatheter Treatments
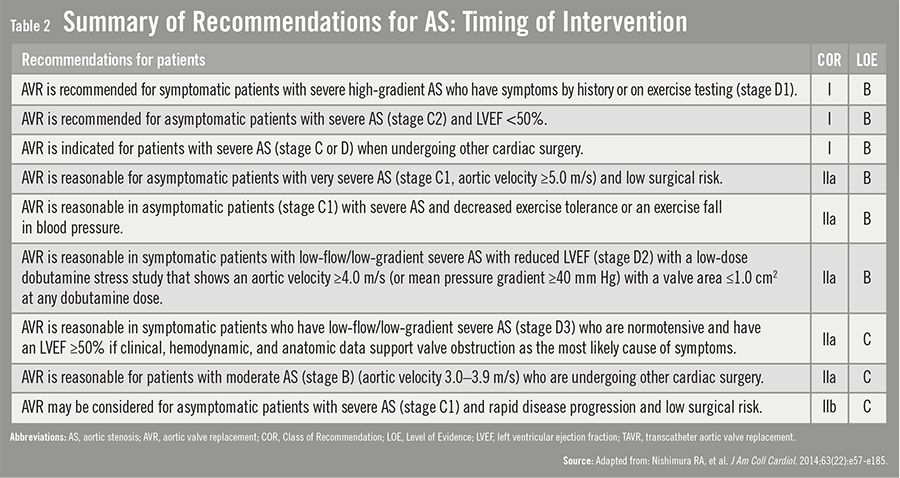
For the first time, the 2014 ACC/AHA guidelines provide a more complex evaluation of interventional risk and indications for newer catheter-based therapies, such as transcatheter aortic valve replace-ment (TAVR). “The introduction of TAVR and other catheter-based therapies has been an important advance but has also made VHD management increasingly complex,” Dr. Sorajja says. To help clinicians discern the risks and benefits of these treatments, the guideline includes recommendations on the timing of these interventions (Table 2).
Other Important Recommendations
The ACC/AHA guidelines also include a recommendation for the use of Heart Valve Teams and Heart Valve Centers of Excellence. “These programs allow for multidisciplinary care of complex patients with VHD,” says Dr. Sorajja. The guideline also provides a lower threshold for surgery to include more patients with asymptomatic severe valve disease. Properly selected patients with severe asymptomatic aortic stenosis and severe asymptomatic mitral regurgitation can now be considered for intervention. Candidacy will depend, however, on other factors, such as operative mortality and the ability to achieve a durable valve repair.
Importantly, the guidelines include formatting enhancements that enable it to be used at the point of care. Decision pathway diagrams and several summary tables have been developed. “Efforts have been made to make these guidelines a living document in that they allow for updates and additions based on the publication of new evidence,” Dr. Sorajja says. This approach to developing guidelines may revolutionize the clinical impact of these recommendations. It can ensure that they are current and allow for seamless integration with electronic medical record systems.
“Research is urgently needed on many aspects of VHD to ensure that patients who already have the disease receive optimal therapy and to prevent it in those at risk,” says Dr. Sorajja. “We need national and international registries and more randomized control trials. We must continuously evaluate outcomes data at each Heart Valve Center of Excellence. The focus should also be on patient-centric care with involvement of patients in decision-making processes.”
 TimH
TimH
{kind=link}
{kind=link}