
Hospital readmissions are important contributors to total medical expenditures in the United States and are an emerging indicator of quality of care. “CMS has started to reduce reimbursement for patients who are rehospitalized early for several conditions, but diabetes currently isn’t one of those diseases,” says Kathleen M. Dungan, MD, MPH. “However, it’s known that diabetes is associated with a higher risk for hospital readmission, and while it may not be the primary reason for admission, it is a frequent comorbidity.” Studies suggest that 20% of patients with diabetes are rehospitalized within 30 days of discharge, and 30% of these individuals are hospitalized more than once a year. There were 7.7 million hospital stays for patients with diabetes in the U.S. in 2008, accounting for 20% of hospitalizations and $83 billion in costs.
Research has shown that rehospitalizations occur disproportionately among socioeconomically disadvantaged groups, including Hispanics and African Americans, those living in lower income areas, and those without private insurance. Other risk factors include previous hospitalizations, extremes of age, and socioeconomic barriers. Failing to acknowledge diabetes at discharge raises the risk of early hospital readmissions, says Dr. Dungan.
Examining the Literature
Some studies have suggested that involving diabetes specialist teams may reduce readmission rates, but results can vary depending on the individual components of the program and attention to discharge needs. Typically, inpatient diabetes management teams incorporate some component of diabetes education, but Dr. Dungan says many hospitals have inadequate funding or resources to optimize this treatment strategy. “Patient education for diabetes is often thought of as being most effective when delivered in the outpatient setting,” she says. “However, barriers to outpatient education—such as access, coverage, and competing medical priorities—are common, and it’s possible that diabetes education in the inpatient setting can further reduce hospital readmissions.”
Benefits of Inpatient Diabetes Education
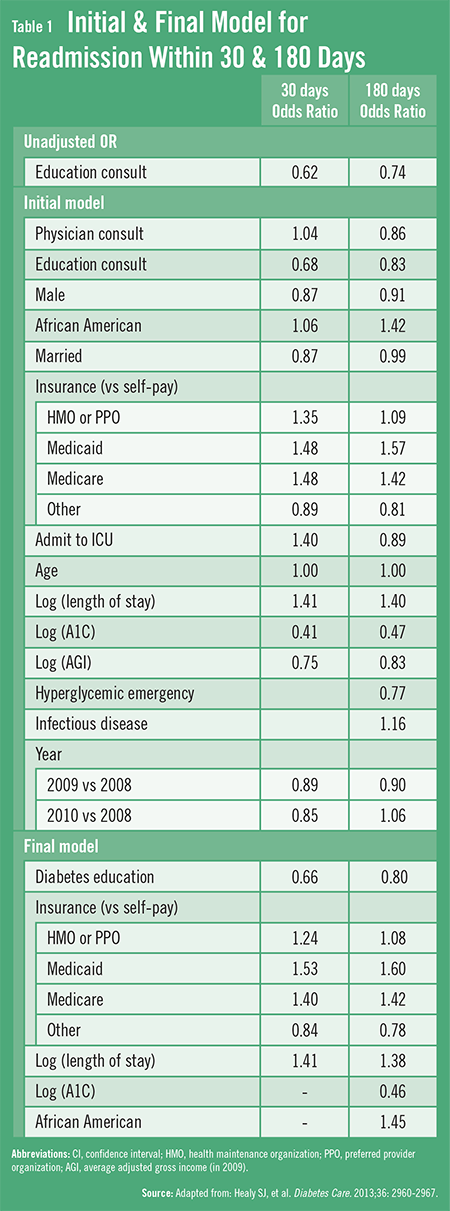
A study published recently in Diabetes Care by Dr. Dungan and colleagues sought to determine whether inpatient diabetes education (IDE) improved the frequency of readmissions in patients with poorly controlled diabetes, which was defined as having an A1C of 9% or higher. The retrospective analysis was done using patient records pulled from the Information Warehouse at Ohio State University. Patients were assessed for readmission within 30 and 180 days after discharge. All patients who received education had an IDE consult order from their physician. IDE was provided by certified diabetes educators and ranged from survival skills focusing on basic diabetes management to more comprehensive education that was individualized following patient assessment.
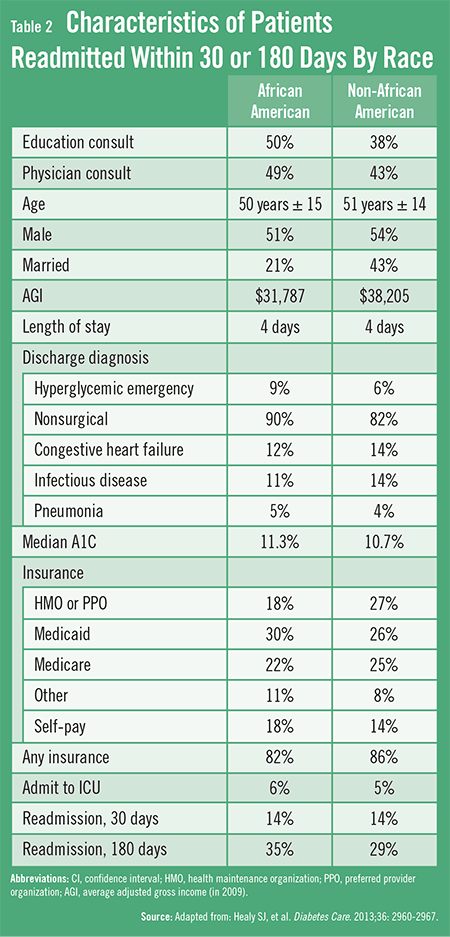
“Even after we controlled for other variables, we found that formal IDE for those with poorly controlled diabetes led to fewer all-cause readmissions,” Dr. Dungan says. IDE was associated with 34% lower odds of all-cause readmissions by 30 days and 20% reduced odds of readmissions by 180 days (Table 1). The study also analyzed data according to race and showed that African Americans were equally likely to be readmitted within 30 days as other races but had a higher readmission frequency within 180 days (Table 2). However, there was a significant reduction in hospital readmissions within 30 days among all races receiving IDE.
“Considering the magnitude of our findings, detailed IDE should be considered as a potentially effective patient management strategy that can be conducted in the hospital,” says Dr. Dungan. “IDE is one of several key drivers of effective hospital discharges among patients with poor glycemic control. Multiple approaches—such as follow-up appointments, medication reconciliation, and patient education—will be necessary to providing the most effective care and to reducing hospital readmission rates for this patient population.” She adds that patients with poor glycemic control stand to benefit the most from IDE.
More Confirmation Needed
Further prospective randomized controlled studies are needed to determine whether actual individualized IDE improves readmission rates and to assess if this approach is cost-effective, according to Dr. Dungan. “Reducing readmissions can reduce healthcare costs and improve quality of care, but we need more data to determine which patient characteristics predict the most benefit from IDE,” she says. More research is also needed to determine the most appropriate content and methodology of such education.
The research by Dr. Dungan and colleagues is one of the largest studies to date to examine the effect of formal IDE on hospital readmissions. “Our finding that patients receiving IDE had significantly lower readmission rates is important when taken in the context of the overall increasing attention that’s being paid to hospital readmissions,” Dr. Dungan says. “If our data are confirmed in future analyses, it’s clear that we’ll need to focus more resources on implementing IDE as an important component of diabetes care.”
 TimH
TimH
{kind=link}
{kind=link}