

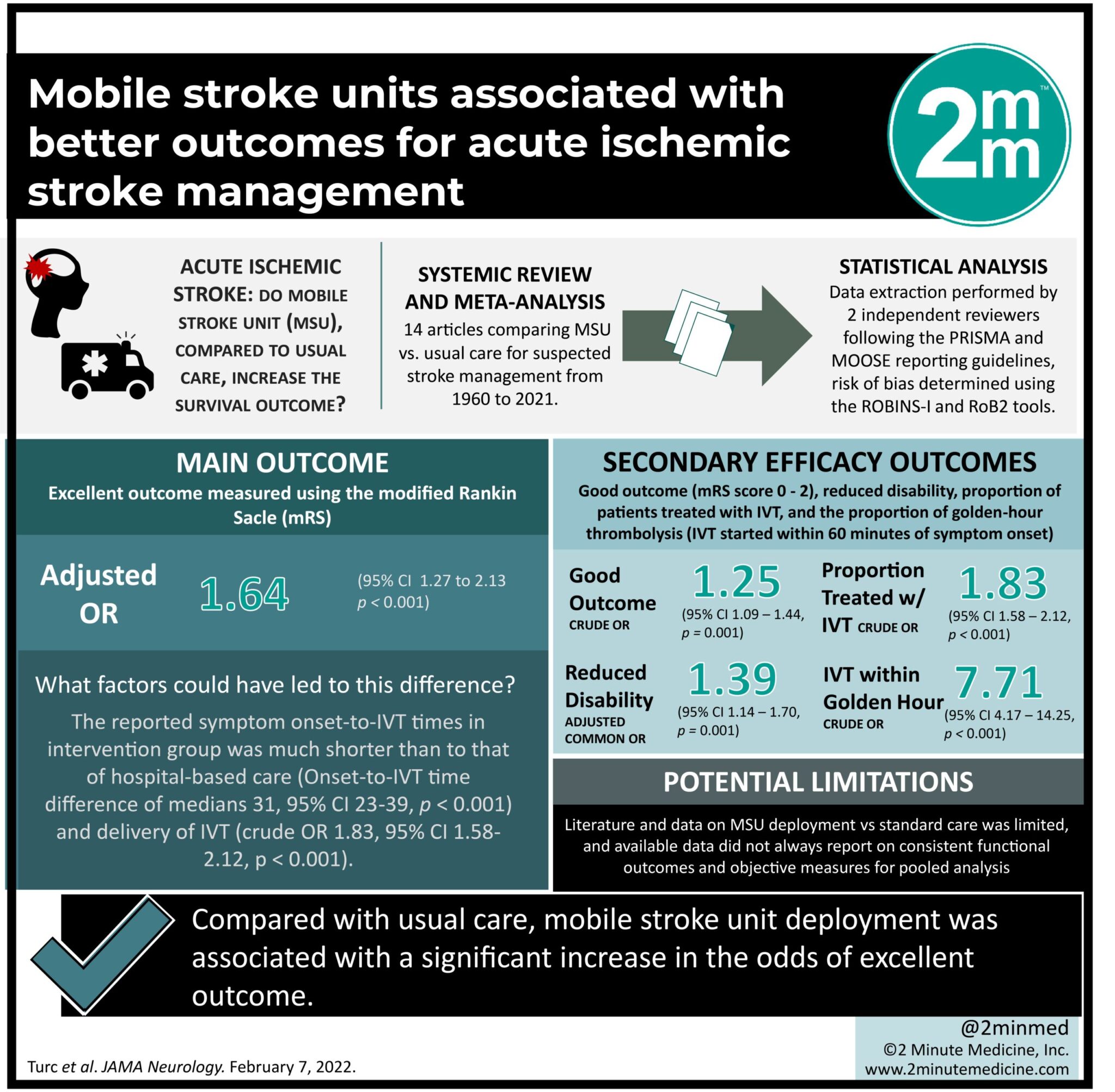
- Compared with usual care, mobile stroke unit deployment was associated with a significant increase in the odds of excellent outcome, a higher proportion of treatment via intravenous thrombolysis, and a 30-minute reduction in onset-to-thrombolysis times, without safety concerns.
- However, it must be recognized that mobile stroke unit implementation is associated with significant costs and requires specialized training and optimal integration into regional emergency response services.
Evidence Rating Level: 1 (Excellent)
Study Rundown: The mobile stroke unit (MSU), largely based on the ‘time-is-brain’ concept in acute stroke, was first implemented in the early 2000s. It involves a specialized ambulance equipped with computed tomography technology, point-of-care laboratory, and neurological expertise to expedite workup and recanalization in acute ischemic stroke. It is now available in several regions across the world; however, uncertainty remains as to whether there is sufficient evidence to suggest better functional outcomes with MSU deployment compared with usual care – especially given the high costs of acquiring and maintaining them. This systematic review and meta-analysis assessed the magnitude of benefit from shifting acute stroke management into the prehospital phase of care with MSUs in comparison with usual care. The main endpoint was excellent outcome measured using the modified Rankin Scale (mRS; score of 0 to 1 at 90 days). Overall, MSU deployment was significantly associated with an approximately 65% increase in the odds of excellent outcome at 90 days, a higher proportion of intravenous thrombolysis (IVT), and a reduction of 31 minutes in onset-to-IVT time, without safety concerns. These findings may help inform clinicians and decision makers in creating safe and evidence-based guidelines on prehospital stroke care. A limitation of this study was that literature and data on MSU deployment vs standard care was limited, as the concept is still relatively recent and has not been widely implemented across the world. Furthermore, available data did not always report on consistent functional outcomes and objective measures for pooled analysis.
Click to read the study in JAMA Neurology
Relevant Reading: Diagnosis and treatment of patients with stroke in a mobile stroke unit versus in hospital: a randomised controlled trial
In-Depth [systematic review and meta-analysis]: This review included 14 articles comparing MSU use vs usual care for suspected stroke management from a search of MEDLINE, Cochrane Library, and Embase between 1960 to 2021. Data extraction was performed by 2 independent reviewers following the PRISMA and MOOSE reporting guidelines and the risk of bias was determined using the ROBINS-I and RoB2 tools. Data were then pooled in random-effects meta-analyses. Compared with usual care, MSU deployment was associated with excellent outcome (aOR, 1.64; 95%CI, 1.27-2.13; P < .001; 5 studies; n = 3228), reduced disability over the full range of the mRS (aOR, 1.39; 95%CI, 1.14-1.70; P = .001; 3 studies; n = 1563), good outcome (mRS score of 0 to 2: crude OR, 1.25; 95%CI, 1.09-1.44; P = .001; 6 studies; n = 3266), shorter IVT times (median reduction, 31 minutes [95%CI, 23-39]; P < .001; 13 studies; n = 3322), delivery of IVT (crude OR, 1.83; 95%CI, 1.58-2.12; P < .001; 7 studies; n = 4790), and IVT within 60 minutes of symptom onset (crude OR, 7.71; 95%CI, 4.17-14.25; P < .001; 8 studies; n = 3351). Additionally, MSU deployment was not associated with an increased risk of all-cause mortality at 7 or 90 days or symptomatic intracranial hemorrhage after IVT.
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.