

According to published research, the use of CT when evaluating adults with blunt trauma injuries has risen dramatically in the past 2 decades. CT can provide clinicians with information about internal injuries, and many trauma centers routinely examine victims of major trauma using head-to-pelvis CT. However, chest CTs do not always provide much additional information if they are completed after a normal chest x-ray. “Chest CTs can expose patients to significant radiation doses that may increase their risk of cancer,” says Robert M. Rodriguez. “Costs associated with chest CT are also high for patients, with a single chest CT scan costing as much as $3,800. In addition, performing these scans can consume large amounts of time for both physicians and patients.”
Developing Helpful Instruments
Considering the potential risks, efforts are needed to reduce the costs and radiation risks of unnecessary blunt trauma imaging. In a study published in PLOS Medicine, Dr. Rodriguez and colleagues sought to derive and validate clinical decision instruments that identify patients with blunt trauma injuries and can therefore help guide the ordering of chest CT. “The purpose of these decision instruments is to empower clinicians to determine when they can safely forego CTs in patients with blunt injuries based on simple, clinical criteria,” Dr. Rodriguez says.
The investigators enrolled 11,477 patients in total, with 6,002 patients in the derivation phase and 5,475 patients in the validation phase. As part of the study, a panel of expert ED physicians and trauma surgeons defined major and minor blunt trauma injuries that were detectable with chest CT. Major injuries included aortic injuries, ruptured diaphragms, collapsed lungs, blood in the pleural chest cavity, and thoracic spine, shoulder blade, and sternum fractures, bruised lungs that required mechanical ventilation, or injuries to the esophagus, trachea, or bronchi of the lungs that required surgery. Minor injuries included other injuries that did not require surgical interventions or mechanical ventilation, such as broken ribs or minor bruising of the lung.
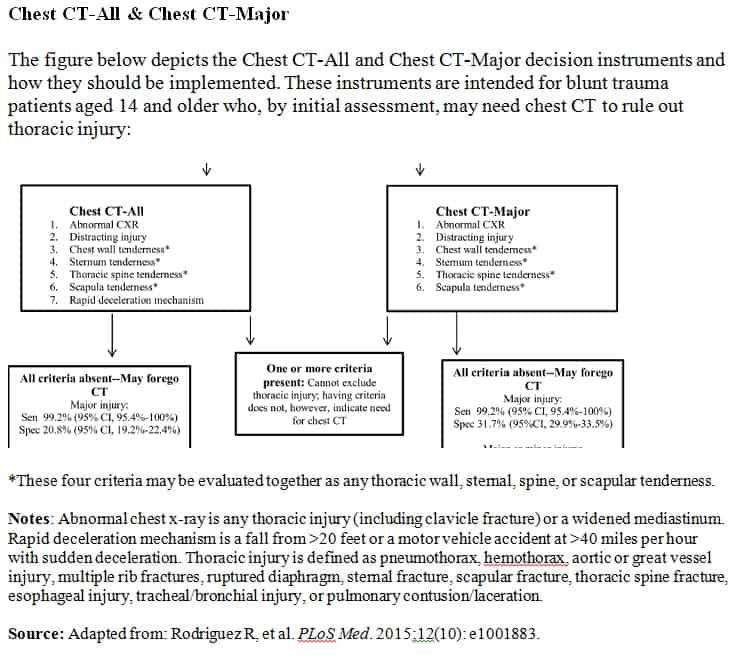
Based on data collected from the derivation phase, the investigators developed the Chest CT-All and the Chest CT-Major decision instruments. Chest CT-All was intended to maximize sensitivity for major and minor chest injuries and consisted of seven clinical criteria, including an abnormal x-ray, rapid deceleration mechanism, distracting painful injury, and bone tenderness of the chest, thoracic spine, and shoulder blade. The Chest CT-Major instrument was intended to maximize sensitivity only for major chest injuries and consisted of the same criteria without the rapid deceleration mechanism (Figure). The study was observational rather than interventional, with trauma care providers in the ED being unaware of the decision-making tools when deciding whether or not to order CTs.
During the validation phase, the researchers determined that the Chest CT-All had a sensitivity of 99.2%, a specificity of 20.8%, and a negative predictive value (NPV) of 99.8% for major injury. Chest CT-All had a sensitivity of 95.4%, a specificity of 25.5%, and a NPV of 93.9% for either major or minor injury. Chest CT-Major had a sensitivity of 99.2%, a specificity of 31.7%, and a NPV of 99.9% for major injury. For major or minor injuries, Chest CT-Major had a sensitivity of 90.7%, a specificity of 37.9%, and a NPV of 91.8%.
Assessing Implications
“These instruments allow clinicians to identify virtually everyone with blunt trauma injuries, enabling us to safely forego CT in patients who do not exhibit any of the decision instrument criteria,” says Dr. Rodriguez. “Clinicians can use physical examinations and history findings instead of imaging to rule out blunt chest injury in many patients attending trauma centers. Use of these decision instruments could reduce the number of unnecessary chest CTs undertaken in trauma centers by up to one-third, thus reducing costs and radiation exposure in people with blunt trauma.”
Dr. Rodriguez notes that clinicians may order CT scans more frequently because of fears of missing injuries and medical-legal concerns. “However,” he says, “by documenting that patients are low risk based on criteria ascertained by these decision instruments, we may be able to counter these fears and legal concerns.” This can be done in a manner similar to the current clinical implementation of the cervical spine and pediatric head trauma rules that have been developed in recent years.
“The clinical criteria we incorporated into the decision-making tools are simple, straightforward components of the routine trauma history and physical exam,” Dr. Rodriguez says. “Hospitals throughout the U.S. can easily implement these decision instruments into their current care protocols. Clinicians should not need to spend more time, money, or effort to implement them.” He notes, however, that it is important for clinicians to recognize that these decision instruments should be used to augment rather than replace clinical judgment.
 PWeekly
PWeekly
{kind=link}