
Cardiac biomarkers have emerged as a powerful tool to rapidly detect an acute coronary syndrome (ACS), but these biomarkers can also be detected in various other illnesses (eg, false-positive result). Throughout the United States, EDs are increasingly using sensitive assays for cardiac biomarkers to diagnose ACS early so that clinicians can initiate potentially life-saving evidence-based therapies in a timely fashion.
Non-traumatic chest pain is a symptom that is typically associated with suspected ACS and ranks among the most common reasons for visits to the ED. However, cardiac biomarker testing is not routinely recommended for all patients who present to the ED. “Most patients who are diagnosed with ACS initially present to the ED with chest pain,” explains Anil N. Makam, MD, MAS. He notes that even with highly sensitive assays, decisions to test for cardiac biomarkers should be considered in the context of patients’ clinical presentation.
“Using cardiac biomarker testing in patients with an extremely low probability of ACS is likely to result in substantial downstream harms from false-positive test results,” Dr. Makam says. “These include patient anxiety, inappropriate additional testing, and unnecessary treatments.” However, it is challenging to estimate the potential extent of harm from false-positive test results because little is known about the current rates of cardiac biomarker testing in EDs.
Assessing Test Use
For a study published in JAMA Internal Medicine, Dr. Makam and Oanh K. Nguyen, MD, MAS, sought to determine the overall use of cardiac biomarker testing and stratified testing by disposition status and selected characteristics. The retrospective study involved adult ED visits that were selected from the 2009 and 2010 National Hospital Ambulatory Medical Care Survey, a probability sample of ED visits in the U.S. Cardiac biomarker tests assessed in the study included creatinine kinase MB, troponin I, and troponin T. ACS-related symptoms were defined broadly to capture all individuals who may have had even the slightest suspicion of ACS (ie, malaise). “We wanted to look at how cardiac biomarker testing is used in EDs and assess patient and visit characteristics that correlated with testing,” says Dr. Makam.
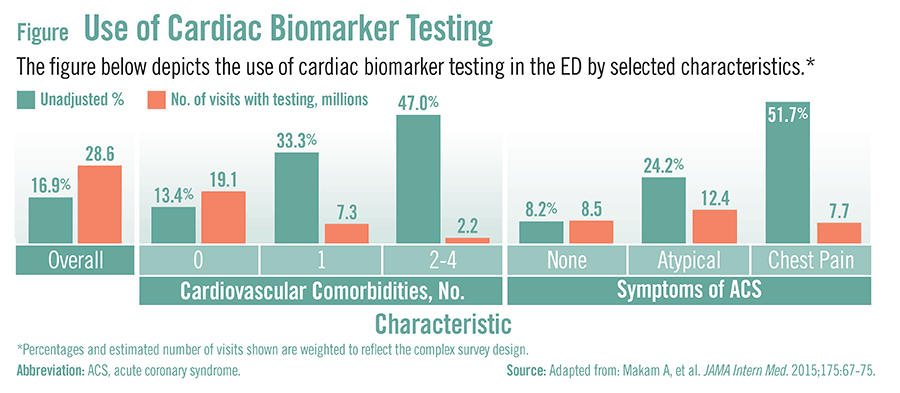
According to the results, cardiac biomarkers were tested in 16.9% of ED visits, representing 28.6 million visits during the 2-year study period (Figure). Cardiac biomarker testing occurred in 8.2% of visits in the absence of ACS–related symptoms, representing 8.5 million visits. “Among visits with cardiac biomarker testing performed, almost one-third had testing in the absence of ACS symptoms.” Dr. Makam says. Among ED patients who were later hospitalized, cardiac biomarkers were tested in 47.0% of all visits. In this patient group, testing of cardiac biomarkers occurred in 35.4% of visits despite the absence of ACS-related symptoms.
Examining Potential Reasons
The study also highlighted several potential reasons why healthcare providers may perform cardiac biomarker testing even in the absence of symptoms that are suggestive of ACS. Increasing patient age and disposition status were significant predictors of cardiac biomarker testing. This suggests that testing occurs disproportionately among patients who are perceived as being sicker.
“The number of other tests or services performed was the strongest predictor of biomarker testing, independent of symptoms of ACS,” says Dr. Makam. When compared with zero to five other tests or services being performed, more than 10 other tests or services being performed was associated with 59.6 times the odds of cardiac biomarker testing.
There are many reasons why high-volume testing may occur. Healthcare providers who order these tests may be fearful of missing a diagnosis and, as a result, order these tests just in case. Pressures to ascertain a quick diagnosis, diagnostic uncertainty, and practice culture are other potential reasons for testing of cardiac biomarkers when there are no symptoms suggestive of ACS.
Considering the Implications
Cardiac biomarkers are extremely useful when tested in patients with suspected ACS. However, testing patients without symptoms suggestive of ACS can lead to harm. “When we extrapolate our findings, our conservative estimate is that there were 1.7 million U.S. patients with a false-positive cardiac biomarker test over our 2-year study period,” Dr. Makam says. “We need to consider the downstream ramifications of inappropriate cardiac biomarker testing, including unnecessary additional tests and treatments. Our study is a first step toward gaining a better understanding of the potential harms of both inappropriate testing and false-positive results. More attention is needed to better characterize these harms and to develop strategies for targeted and appropriate use of cardiac biomarker tests in the ED setting.”
 Janine Anthes
Janine Anthes
{kind=link}