

Evidence suggests that several obstacles appear to prevent widespread acceptance of electronic health records (EHRs) among many physicians, including allergists and immunologists. However, several potential solutions may enable providers to benefit from EHR technology.
The United States government has made multiple efforts to promote more widespread adoption of electronic health records (EHRs), including the $35 billion Health Information Technology for Economic and Clinical Health (HITECH) Act. Despite these efforts, results from several surveys suggest that physician satisfaction with, and adoption of, EHRs remains low.
Thorough analyses on the current status of EHR use and the barriers keeping physicians, including allergists and immunologists, from adopting fully functioning EHR systems are lacking. “To date, there are no scholarly articles evaluating the use of fully functional EHRs from the perspective of an allergist or immunologist,” says Lawrence D. Frenkel, MD. For a review published in Allergy and Asthma Proceedings, Dr. Frenkel explored the goals of optimal EHRs, the reasons behind the lack of widespread adoption, and potential solutions to these problems.
The Optimal EHR
“Locating specific information within paper records of complicated patients can be time-consuming and fraught with errors,” explains Dr. Frenkel. “Some information may not be recorded correctly, if at all, or may be difficult to find. EHRs, however, provide a template for completeness in the physical examination. Those who access carefully completed EHRs can easily see what physicians do and find as well as what was not done. For example, vital signs can be easily recorded and viewed longitudinally in EHRs. Current medications, their indications, and the clinicians who prescribed them are also easily accessed in an EHR. When pharmacists have access, healthcare providers can quickly see what prescriptions have been ordered and delivered.”
One of the biggest promises of optimal EHRs is the concept of interoperability, or the ability of EHR systems to share information with one another, allowing authorized clinicians to view and update the primary records of any patient using their own system, regardless of what system was used to create the record. “Interoperability can improve quality of care by preventing duplicate tests or procedures or the administration of contraindicated medications,” says Dr. Frenkel.
Dr. Frenkel notes that optimal EHRs can also prominently list a patient’s allergies and automatically create warnings if clinicians prescribe something to which patients are supposedly allergic. When seeing new patients, allergists can focus on this component of the EHR and evaluate if allergies are truly present while also double checking historical details. With EHRs, immunologists can follow important laboratory details longitudinally to better understand more about the true immunologic status of patients over time.
Barriers to Well-Functioning EHRs
“Few scientific studies have been conducted in support of the assumption that EHRs save money and lives and result in better care when compared with standard paper records,” says Dr. Frenkel. “There’s a real cost to initiating EHRs, from buying software and hardware to training users and maintaining the system. Physicians now know that using EHRs can add a considerable amount of time to their tasks.”
The mandated technology under HITECH is potentially oppressive, according to Dr. Frenkel, and the quality of EHR systems often does not meet these demands. The goal of achieving interoperability is not materializing like many have hoped, primarily because EHR developers are in competition with one another and have few incentives to create interoperable systems. Also, the software for most EHR systems was written without specialists in mind. “Specialists often struggle with systems that don’t offer a clear advantage over paper records or meet their needs,” Dr. Frenkel says.
The creation and population of an EHR can detract from physician–patient interactions. Healthcare providers who spend the vast majority of their time with patients using and populating data on the computer may not pick up on patients’ body language. This can lead them to miss out on opportunities to pursue new leads in terms of the patients’ health history.
Potential Solutions
Dr. Frenkel notes that there are several possible solutions to improving EHR acceptance (Table below), and recommends that data entry for EHRs be user-friendly, clear, and to-the-point to help meet expectations. “An ideal EHR would allow users to enter specifically what was done during patient visits into the system, which would then populate this information into a standard format rather than requiring clinicians to check boxes,” says Dr. Frenkel. He adds that incorporating dictation software into EHRs—without the burden of keyboard data entry—would help with adoption and ease of use.
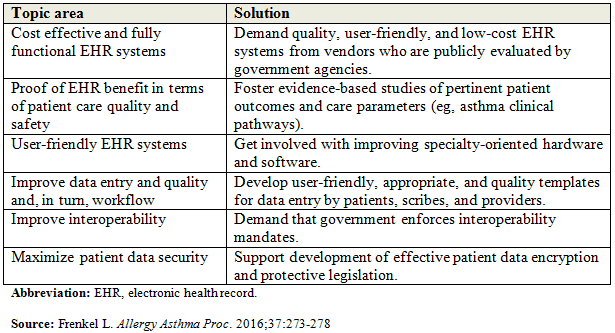
Potential Solutions for Improving EHR Acceptance.
“The government that is pushing EHR use has to enforce the requirement that they be fully functional and interoperable,” says Dr. Frenkel. “With the help of various medical societies, clinicians can and should demand what they want and need in their EHRs. “The government needs to step up and create regulations to meet these demands and vendors should strive to develop software that works for our specific needs.”
Lawrence D. Frenkel, MD, has indicated to Physician’s Weekly that he has no financial interests to disclose.
 PhysWeekly
PhysWeekly