

Hypertriglyceridemia can substantially increase the likelihood of patients developing heart disease when compared with those who have normal triglyceride levels. While treatment strategies for this condition are well established, its causes differ from patient to patient, as do the risks they pose to each individual. Clinical practice guidelines from the Endocrine Society on hypertriglyceridemia were published in the September 2012 Journal of Clinical Endocrinology and Metabolism (view and print guideline summary here). They recommend that more attention be paid to how personal history, physiology, and lifestyle interact to affect risk.
“In recent years, much of the focus surrounding lipids has concentrated on cholesterol,” explains Lars Berglund, MD, PhD, who chaired the Endocrine Society task force that developed the most recent guidelines. “Although there are evidence–based guidelines from respected medical associations that address lipids, data on the complex role of triglycerides in heart disease continue to accumulate. Considering this recent emergence of data on triglycerides, it was important to focus on a guideline that specifically discusses this component of heart disease care.”
Individualized Approach with Elevated Triglycerides
Dr. Berglund stresses that clinicians should not view elevated fasting triglyceride levels as a standalone factor. “Triglycerides should be looked at in the context of other risk factors for cardiovascular disease (CVD) and metabolic disease,” he says. “Assessment should include the evaluation of secondary causes of hyperlipidemia, including endocrine conditions and medications [Table 1]. Central obesity, hypertension, abnormalities of glucose metabolism, liver dysfunction, and family history of dyslipidemia and CVD should be assessed.” For example, patients with triglyceride levels in the moderate range—200 mg/dl to 999 mg/ dl—may have changes in HDL and LDL cholesterol levels and properties, which are associated with cardiovascular risk, but insulin resistance and other factors should also be considered during patient management. Patients with isolated hypertriglyceridemia (eg, familial type) are more likely to have larger particles, which are less likely to cause cardiovascular risk.
Fatty foods, smoking, and poor exercise also contribute to the risk for high triglyceride levels. “Simple carbohydrates that can be broken down and absorbed quickly, such as sugar-sweetened beverages, white rice, and white bread, contribute to an increase in fat formation and triglyceride levels,” says Dr. Berglund. While alcohol can increase HDL cholesterol levels, it can also lead to high triglyceride levels. Certain prescription medications (eg, bile acid sequestrants for high LDL) can also interact to raise blood triglyceride levels. “Understanding the importance of specific risk factors requires that clinicians ascertain a full profile of each patient,” Dr. Berglund adds.
Considering Treatment Options for Hypertriglyceridemia
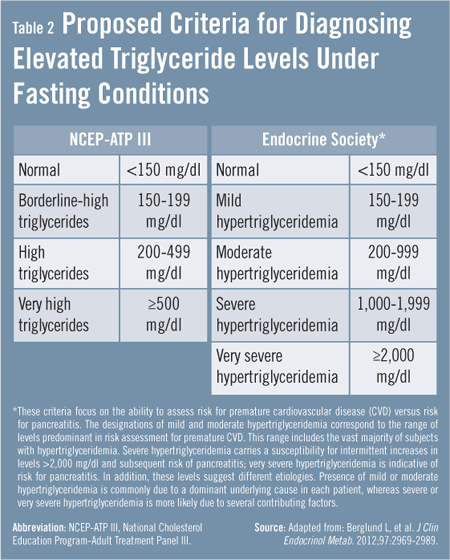
Defining the level of hypertriglyceridemia for individual patients is crucial to determining the goal of treatment and should be based on fasting levels. The Endocrine Society guidelines define normal triglyceride levels as less than 150 mg/dl (Table 2). Mild and moderate hypertriglyceridemia are categorized by levels below 999 mg/dl, which are primarily associated with a risk for CVD. When levels rise above 1,000 mg/ dl, patients should be categorized as having severe and very severe hypertriglyceridemia. The risk for these individuals is associated more often with pancreatitis.
Because weight, diet, and exercise play particularly important roles in triglyceride levels, the Endocrine Society guideline recommends that initial treatment for mild-to-moderate hypertriglyceridemia be lifestyle therapy, consisting of dietary counseling, physical activity, and a weight reduction program for overweight and obese patients. “Overweight or obese patients may feel overwhelmed when asked to lose weight,” Dr. Berglund says, “but clinicians should reassure them that even modest reductions in weight can have highly beneficial effects on their triglyceride levels.”
For patients at risk for triglyceride-induced pancreatitis and for whom lifestyle changes have been ineffective, the guideline recommends that fibrates be used as the first-line of drug treatment. Although statins have some triglyceride-lowering effects, they are not overly effective in patients with very high levels, according to Dr. Berglund. The guideline recommends that statins not be used as monotherapy for severe or very severe hypertriglyceridemia, but may be useful for moderate hypertriglyceridemia when indicated to modify cardiovascular risk. Fibrates, niacin, and n-3 fatty acids are recommended for use alone or in combination with statins in patients with moderate-to-severe triglyceride levels.
“The key take-home message for all clinicians is that patients with high triglyceride levels need to be evaluated for secondary causes on an individualized basis,” says Dr. Berglund. “Only then can we determine the causes and direct our focus of treatment. The Endocrine Society guidelines can serve as a helpful aid for physicians as they manage patients from diagnosis to treatment.”
 JonN
JonN
{kind=link}
{kind=link}