
In recent decades, physicians have used the male model of testing to identify coronary artery disease (CAD) in women, but studies show that there are gender-specific differences in the pathophysiology of coronary atherosclerosis. “These differences are multifactorial and include obstructive and non-obstructive CAD as well as dysfunction of the coronary microvasculature and endothelium,” explains Jennifer H. Mieres, MD, FACC, FASNC, FAHA. “As such, the term ischemic heart disease (IHD) best describes the varied pathophysiology in women. Women with IHD are at increased risk for coronary events.”
Using the male model approach has led to under-diagnosis and under-treatment of IHD for women, which in turn has led to higher case fatality rates and greater morbidity. More recently, efforts have been made to ensure gender equality in the quantity and quality of research by better representing women in clinical trials and registries. These efforts were made to optimize management strategies for women with suspected and known IHD.
A New Consensus on Coronary Artery Disease in Women
In 2005, the American Heart Association (AHA) published a consensus statement on the use of CAD imaging for evaluating symptomatic women with suspected myocardial ischemia. Since that time, many reports have provided additional high-quality evidence, including data on coronary CT angiography (CCTA) and cardiac MRI (CMR). In 2014, the AHA updated this statement and published it in Circulation. The update provides sex-specific data on the diagnostic and prognostic accuracy for exercise treadmill testing (ETT) with electrocardiography, stress echocardiography, stress myocardial perfusion imaging (MPI) with single-photon emission CT or positron emission tomography, stress CMR, and CCTA.
“In the past, clinicians didn’t recognize the importance of non-obstructive CAD in women,” says Dr. Mieres, who was co-chair of both the 2005 and 2014 AHA consensus statements. “This led to false-positive stress tests and a lack of appropriate treatment. We now recognize that women experience a broader range of IHD symptoms than men and have a different pattern and distribution of pain symptoms. Women may present with the classic symptoms of left-sided chest pain or pressure, but other symptoms that aren’t localized to the chest may also present. These include jaw pain, upper back pain, and widespread indigestion. In addition, women’s symptoms are frequently associated with mental or emotional stress, whereas men’s symptoms are more likely to result from physical exertion.”
Key Recommendations from the AHA Consensus
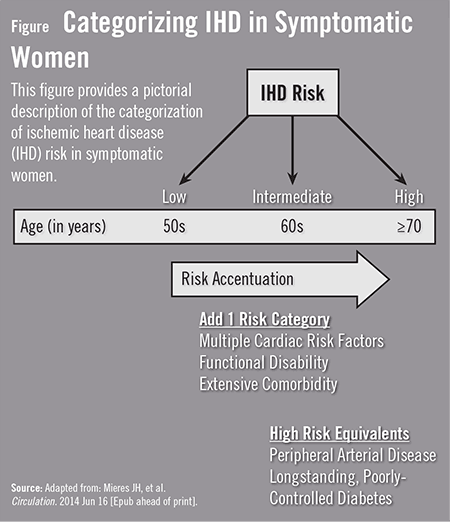
The most recent AHA consensus statement provides helpful diagnostic recommendations for women presenting with suspected IHD symptoms and for establishing the level of IHD risk (Figure). “Healthcare providers should determine whether a woman is at low, intermediate, or high risk for IHD and discuss the available options,” Dr. Mieres says. “The level of risk should help steer these conversations on which diagnostic tests to use.”
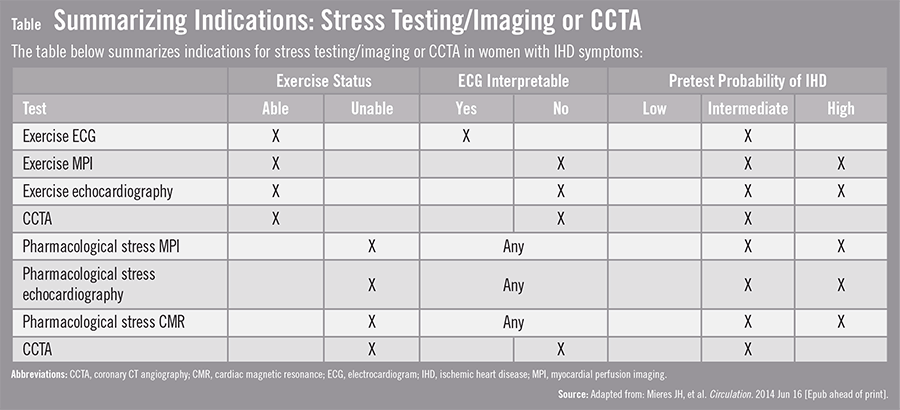
According to the consensus statement, low-risk women are not candidates for diagnostic testing in most cases. Women at low and intermediate IHD risk are recommended to first undergo a treadmill exercise electrocardiogram (ECG). For symptomatic women with functional disability, an indeterminate ETT, or an abnormal rest ECG, the AHA recommends echocardiography or MPI; CMR may be considered a reasonable test option. CCTA may also be considered reasonable for women at intermediate IHD risk. The AHA writing group developed a summary of recommendations for IHD imaging in women with ischemic symptoms (Table).
Ischemic Heart Disease: Important Caveats
According to the AHA, there are several caveats to consider when discussing the risks and benefits of diagnostic tests with women suspected of IHD. For example, women of childbearing age may want to avoid tests that require exposure to radiation. “We must also consider a woman’s functional ability when determining the type of diagnostic testing to use,” says Dr. Mieres. “Women with low functional disability are at higher risk for heart attacks.”
Premenopausal women at intermediate IHD risk who are functionally disabled generally are recommended to undergo echocardiography or CMR. However, they may also be candidates to undergo MPI or CCTA if an effective radiation dose of less than 3 mSv is possible. When stratifying risk, clinicians are urged to base their decisions on the extent and severity of inducible abnormalities noted on the stress examination.
Dr. Mieres says that the most recent AHA consensus statement update allows clinicians to better determine the risks and treatment strategies for IHD in symptomatic women who were previously undiagnosed. However, she notes that more research is still warranted. “We need additional comparative effectiveness studies to further improve and guide testing,” she says. “The treatment of women presenting with ischemic symptoms is an important aim for future research.”
 TimH
TimH
{kind=link}
{kind=link}