
#PWChat: Why Digital Health Startups Fail & Why Physicians Should Care
Join us April 20 at 3:00PM EST for a live, interactive tweetchat with Meghana C. Karande, MD, on...
Read More
Join us April 20 at 3:00PM EST for a live, interactive tweetchat with Meghana C. Karande, MD, on...
Read More
Artificial intelligence (AI) has begun to achieve its potential by focusing on the major...
Read More
Join us February 26 at 2:00PM EST for a live, interactive tweetchat with Linda Girgis, MD, on what...
Read More
Despite substantial national investment in electronic health records (EHRs) under the HITECH Act,...
Read More
A recent Accenture report found that patients in the United States are increasingly accessing...
Read More
An epidemic is sweeping the country, and no one is doing anything about it. No it’s not Zika...
Read More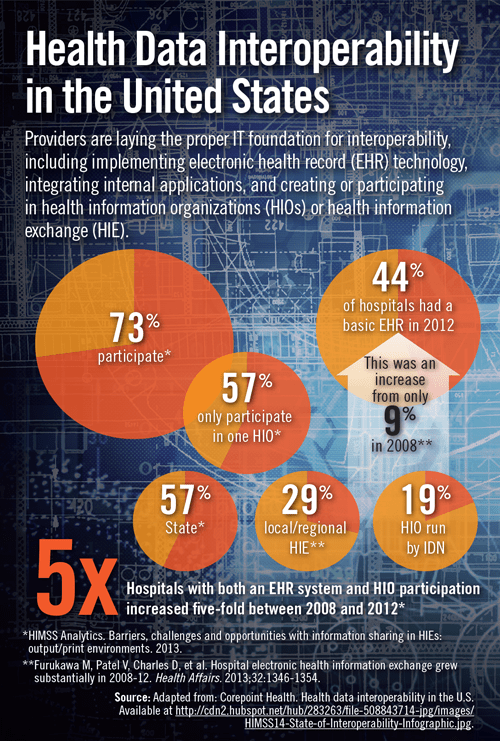
Health Data Interoperatbility in the United States
Read More

Throughout the United States, emergency department information systems (EDISs) have been developed...
Read More
OK, I’ll admit it: I had no idea. I thought that the whining and griping by other doctors about...
Read More
With the emergence of electronic health records (EHRs) and administrative and professional...
Read MoreMost practices, especially smaller ones, do not appear to achieve positive returns on investment when adopting electronic health records (EHRs) with current meaningful use incentives alone. American researchers who surveyed...
Read More
The costs associated with hospital readmission within 30 days of discharge are high. CMS and other...
Read MoreThere are many interesting unintended consequences of electronic medical records (EMRs). I was reminded of this by a recent blog I wrote about what interns really do when they are on call. According to a study from a VA hospital...
Read MorePatients are well ahead of providers in demanding online access to health information (IT) and communication tools, according to a new survey. Consumers are eager to use both the internet and mobile devices to connect with their...
Read MoreOK, I am an EMR geek who isn’t so thrilled with the direction of EMR. So what, I have been asked, would make EMR something that is really meaningful? What would be the things that would truly help, and not just make more hoops...
Read More
This July marked the 16th anniversary of the installation of our electronic medical record. Yup....
Read More
Data theft and compromise in healthcare are on the rise, and the mobile landscape is further...
Read MoreImplementation of a commercially available electronic health record (EHR) appears to improve diabetes care and outcomes, according to results of an American investigation. Patients who were exposed to EHRs were significantly...
Read More
Much of health information technology (IT) focuses on patient documentation, compliance, and...
Read More