

Intra-abdominal injuries resulting from blunt torso trauma are a leading cause of morbidity in children and account for a significant number of ED admissions each year. Identifying these injuries early is critical to reducing morbidity and mortality from delayed or missed diagnoses. In recent years, CT has become standard for diagnosing many traumatic injuries, including those within the abdomen. At the same time, however, CT use in trauma and emergency care has expanded much faster than evidence for its use.
“CT provides detailed and useful information about injuries and helps clinicians make informed management decisions,” explains James F. Holmes, MD, MPH, “but it also has its drawbacks. It exposes patients to relatively large radiation dosages, putting them at risk for radiation-induced malignancies.”
Testing a Prediction Rule on Blunt Torso Trauma
Recently, several smaller investigations have suggested that children with blunt torso trauma can be stratified by risk for intra-abdominal injury using a combination of readily accessible clinical factors. These studies, however, have been limited by their retrospective or single-center study designs and small samples. In an effort to overcome these limitations, Dr. Holmes and colleagues had a study published in Annals of Emergency Medicine that aimed to derive a prediction rule that identifies children with blunt torso trauma for whom CT would generally not be indicated.
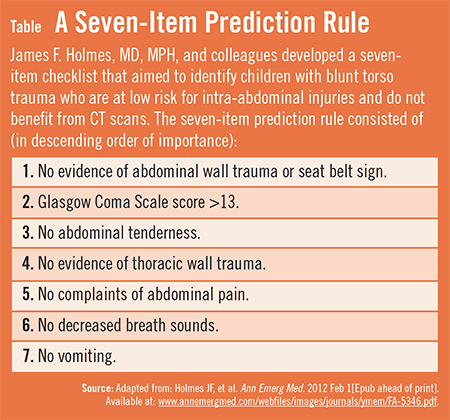
More than 12,000 children (average age, 11.1 years) from 20 EDs with blunt torso trauma were enrolled in the prospective analysis by Dr. Holmes’s study team. A prediction rule was created using a seven-item checklist that included patient history and physical examination variables readily available without the need for using laboratory or ultrasound data (Table).
{kind=link}
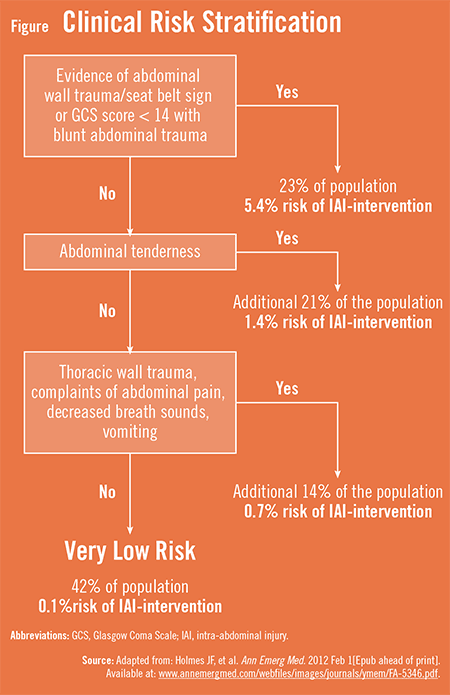
According to the results, the prediction rule correctly identified children with blunt torso trauma who were at very low risk of intra-abdominal injuries undergoing acute intervention. Clinicians identified almost all children with intra-abdominal injury undergoing acute intervention. The risk of intra-abdominal injury undergoing acute intervention rose as the number of variables increased. Patients with blunt abdominal trauma and decreased mental status or physical findings of abdominal wall trauma were at highest risk for intra-abdominal injury, according to the rule. Children without any historical or physical examination findings in the prediction rule were at very low risk (0.1%) for intra-abdominal injury undergoing acute intervention. “Therefore,” Dr. Holmes says, “abdominal CT is generally not warranted for these patients.”
Furthermore, 23% of the abdominal CT scans performed were performed in very-low-risk patients (Figure). “This suggests that there is potential to avoid unnecessary abdominal CT scans in children after blunt torso trauma,” adds Dr. Holmes. “In turn, we can reduce the amount of radiation certain children receive and cut costs associated with CT while still accurately diagnosing and treating these injuries.”
{kind=link}
Important Caveats to Prediction Rules
The prediction rule requires external validation before it can be implemented more widely, says Dr. Holmes. “The checklist relies on the clinical exam and judgment of attending emergency physicians. It doesn’t, however, mandate which children should undergo abdominal CT. Prediction rules are intended to aid and empower clinicians by providing evidence with regard to risk but must be used in conjunction with sound clinical judgment to provide optimal care. For children who aren’t at low risk (eg, are positive for one of the variables), the rule is meant to assist clinicians by providing evidence to aid clinical decision making.” Many who are positive for the rule can still be managed without CT scanning.
Importantly, Dr. Holmes’s study team recommends that clinicians carefully consider which children may benefit from screening laboratory tests or focused assessment sonography for trauma. All patients being discharged from the ED should be provided with proper instructions about indications to return for medical care. Patients admitted for other injuries should also be carefully assessed for intra-abdominal injury to avoid complications that can occur after a missed or delayed diagnosis.
Reducing Radiation in Younger ED Patients
“Emergency physicians are continuing to search for ways to safely reduce the amount of radiation that younger ED patients receive,” Dr. Holmes says. “Our prediction rule could help us accomplish this goal. Patient history and physical examination variables in the prediction rule are available to all clinicians who evaluate injured children in the ED, regardless of location and resources. This enhances the generalizability of our study results and the applicability of the rule to many clinical settings. With further validation, it’s hoped that our prediction rule will lead to more appropriate, evidence-based ED evaluations and resource use.”