

According to the American Diabetes Association, cardiovascular disease (CVD) is the major cause of morbidity and mortality for people living with diabetes. “The common conditions that coexist with type 2 diabetes, such as hypertension and dyslipidemia, are clearly risk factors for CVD,” explains Robert H. Eckel, MD. “Diabetes itself confers additional risk for CVD, including coronary heart disease, stroke, peripheral vascular disease, and heart failure. Obesity, metabolic syndrome, and inflammation are other key components to the link between diabetes and CVD.”
“Large benefits are seen when multiple CVD risk factors are addressed globally.”
Published analyses have shown that controlling individual CVD risk factors helps to prevent or slow CVD in people with diabetes. “Large benefits are seen when multiple CVD risk factors are addressed globally,” says Dr. Eckel. “Clinical trials have shown that lowering glucose aggressively can further help reduce CVD risk, but an individualized approach is necessary for most patients with diabetes.”
Individualizing Care for Diabetes
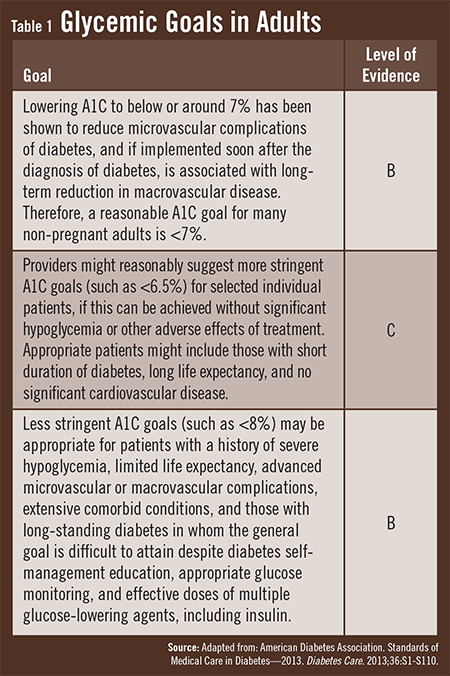
The American Diabetes Association recommends an A1C of less than 7% for most patients, but Dr. Eckel notes that A1C goals may differ from patient to patient, depending on their individual characteristics (Table 1). “There are several aspects to consider when selecting a target A1C level, including age, duration of diabetes, the extent of diabetes complications,
psychosocial support, physical activity limitations, and risks of hypoglycemia. All of these factors—and other cardiometabolic components—will play a role in guiding how aggressively diabetes should be treated.”
Blood Pressure & Cholesterol
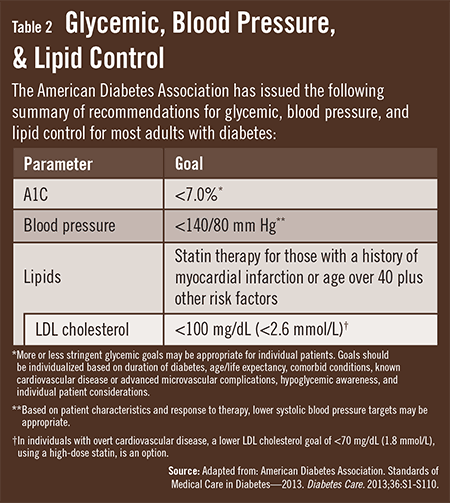
In addition to glycemic control, the management of blood pressure and cholesterol is important to helping prevent or slow CVD in patients with diabetes (Table 2). The American Diabetes Association recommends a blood pressure of 140/80 mm Hg for individuals at risk for CVD if they are currently taking medications. Dr. Eckel notes that most of these patients should also be on an ACE inhibitor or angiotensin II receptor blocker to protect them from kidney disease.

With regard to cholesterol, many adult patients with diabetes will benefit from being on a statin, unless they are contraindicated for such treatment. “Contraindications for higher-dose potent statins include statin intolerance as well as pregnancy, intended pregnancy, or nursing,” Dr. Eckel says. “Higher-dose potent statins can reduce the risk of CVD events by 20% to 25% for people with diabetes, and for those with statin intolerance, lower-dose statins may be tolerated and still somewhat beneficial.”
Other medications are often necessary to reduce the risk of future CVD events. For example, low-dose aspirin can be beneficial when used in patients with diabetes who do not have known CVD. “Aspirin is definitely recommended for those with CVD and diabetes,” says Dr. Eckel. “Those with existing CVD who have previously received stents should also take aspirin and a second antiplatelet agent, such as clopidogrel. These patients should continue taking this dual antiplatelet therapy for at least 1 year, but clinicians should be vigilant and monitor patients for bleeding risks.”
Addressing Lifestyle to Manage CVD Risk
Lifestyle modifications are a critical aspect to managing CVD risk in patients with diabetes. “Clinicians should get a dietary history that indicates how many servings of fruits, vegetables, and whole grains patients eat daily and how many servings of fish patients eat per week,” Dr. Eckel says. “The quality of diet is important. Referral to a diabetes self-management educator or dietitian may be helpful. Setting goals for body weight, modifying food intake, and reducing calories consumed per day are paramount to weight reduction. Ultimately, clinicians need to pay attention to the quality and quantity of diet.” He adds that it is also important to determine if patients may be candidates for weight loss medications or bariatric surgery.
After focusing on dietary issues, Dr. Eckel says that clinicians should address physical activity. “Prescriptions for exercise should be constructed in ways that align with good heart health. Getting patients to exercise is challenging, but any positive encouragement may lead them to become more physically active. For patients who rarely exercise, even 10 to 15 minutes of walking can be of benefit.” Dr. Eckel notes that before writing exercise prescriptions, clinicians should consult with cardiologists if they’re unsure if exercise may harm heart health.
Making Connections Between CVD & Diabetes
While progress has been made in making connections between CVD and diabetes, Dr. Eckel notes that many unanswered questions remain on optimizing care. “For example, it’s unknown if the level of glycemia should be a consideration for clinicians when deciding on the dose of aspirin or if a second antiplatelet drug is necessary. In addition, we’re not sure yet if patients with diabetes and high triglycerides benefit when fibrates are added to statins, or if anti-inflammatory drugs can benefit patients with or without diabetes. Trials are being initiated to address these research gaps and should be of great interest to clinicians as we seek to improve patient outcomes.”
 admin
admin
{kind=link}
{kind=link}