

In recent years, CMS has invested heavily in policies, incentives, and other interventions to encourage healthcare providers to improve transitions in care and reduce avoidable readmissions. Studies have shown that many patients return to the hospital via the ED within 30 days of discharge, but specifications for measuring rehospitalization vary. “Unless patients are readmitted to the hospital through the ED, they aren’t being counted in measurements of readmissions,” says Kristin L. Rising, MD. “By limiting the focus to inpatient-to-inpatient events and omitting ED visits, we’re missing a substantial source of healthcare utilization that is managed solely in the ED.”
Patients may be effectively stabilized and discharged from the ED shortly after hospital discharge, but few data are available on the frequency and cost of ED visits after such discharges. Previous analyses have found that 40% of patients who sought acute medical care had multiple visits for inpatient or ED stays. About one-quarter of these patients had multiple inpatient stays, whereas one-third had multiple ED treat-and-release visits.
Taking a Comprehensive Approach to Readmission Factors
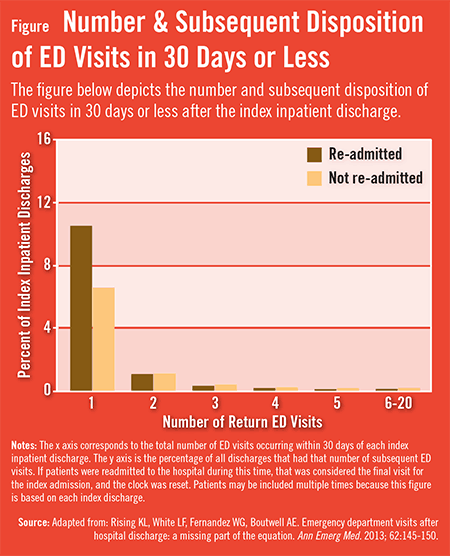
According to Dr. Rising, a comprehensive approach to understanding the factors that contribute to subsequent healthcare use in the post-hospital discharge period should include a closer look at ED use within 30 days of hospital discharge. In a retrospective study published in Annals of Emergency Medicine, Dr. Rising and colleagues examined 15,519 patient discharge records over a 5-month period. Nearly one-quarter (23.8%) of these discharges resulted in at least one ED visit within the subsequent 30 days, and more than half (54.0%) of these visits resulted in discharge back home. The median number of ED visits per patient who sought care within 30 days of discharge was one (Figure).

Among patients who returned for care, the median time to the first return visit was shorter for patients who were readmitted when compared with for patients who were not readmitted from their return ED visit. The primary discharge diagnosis with the highest number of discharges linked to an ED visit within 30 days was non-specific chest pain. Non-hypertensive congestive heart failure was the diagnosis with the highest rate of return ED visits and the highest rate of 30-day readmissions (Table).
Increasing Pressure on EDs to Improve Transition
Many efforts to improve transitions of care are measured according to whether patients are readmitted to inpatient hospital stays within 30 days. “With the implementation of such measures, emergency physicians will be under increasing pressure to find alternatives to admitting patients,” Dr. Rising says. “Tracking the frequency with which patients are returning to EDs after they’re discharged from the hospital may help emergency physicians play a vital role in breaking the readmission cycle.”
“By including ED visits, we can get a more accurate assessment of where care transitions can be improved and how recurrent hospital utilization can potentially be avoided.”
As efforts to improve care transitions evolve, measuring the rate of ED visits after inpatient discharge may provide opportunities for improving care transitions and reducing avoidable acute-level use. “Excluding return visits to EDs from initiatives aimed at reducing recurrent hospital utilization can lead us to miss over half of all returns to acute levels of care after discharge,” says Dr. Rising. “By including ED visits, we can get a more accurate assessment of where care transitions can be improved and how recurrent hospital utilization can potentially be avoided.”
More Work Needed to Establish Alternatives to Readmission
Hospitals and healthcare systems are increasingly implementing strategies to improve care coordination and may consider establishing alternatives to hospital readmission for patients seeking emergency care within a 30-day window of hospital discharge. “In future studies,” Dr. Rising says, “it will be helpful to evaluate what our data imply in terms of priorities about different outcomes. For example, time to return ED visit after inpatient discharge appears to be shorter for patients readmitted to the hospital than for those treated and released from that return visit. Regarding discharge diagnoses, after congestive heart failure, the top diagnoses associated with return ED visits leading to subsequent readmission versus subsequent discharge diverged. Thus, initiatives developed to address recurrent hospital use may need to vary depending on the types of recurrent visits being targeted.”
Hospital and cross-continuum quality improvement teams should consider including ED visits as an important outcome, says Dr. Rising. “Gathering this type of data can reflect progress in improving transitions from hospitals to the next care setting. ED providers should take an active role in collaborating with inpatient, post-acute, and community-based care providers to improve transitions of care and reduce avoidable hospital use. With EDs becoming the primary source of hospital admissions for more Americans, part of the solution to reducing the readmission problem will rest with the ED clinicians who make decisions about whether or not to admit patients.”
 admin
admin
{kind=link}