

A full 85% of patients with aortic stenosis who underwent surgical aortic valve replacement (SAVR) were at low surgical risk according to EuroSCORE assessment, and survival was high—not only in patients with higher risk and older age but also and especially in low-risk patients <70 years old, who had a median survival of more than 15 years. Study results were published in the Journal of the American College of Cardiology.
Further, researchers found that the association between five-year mortality and age was only significant among low-risk patients.
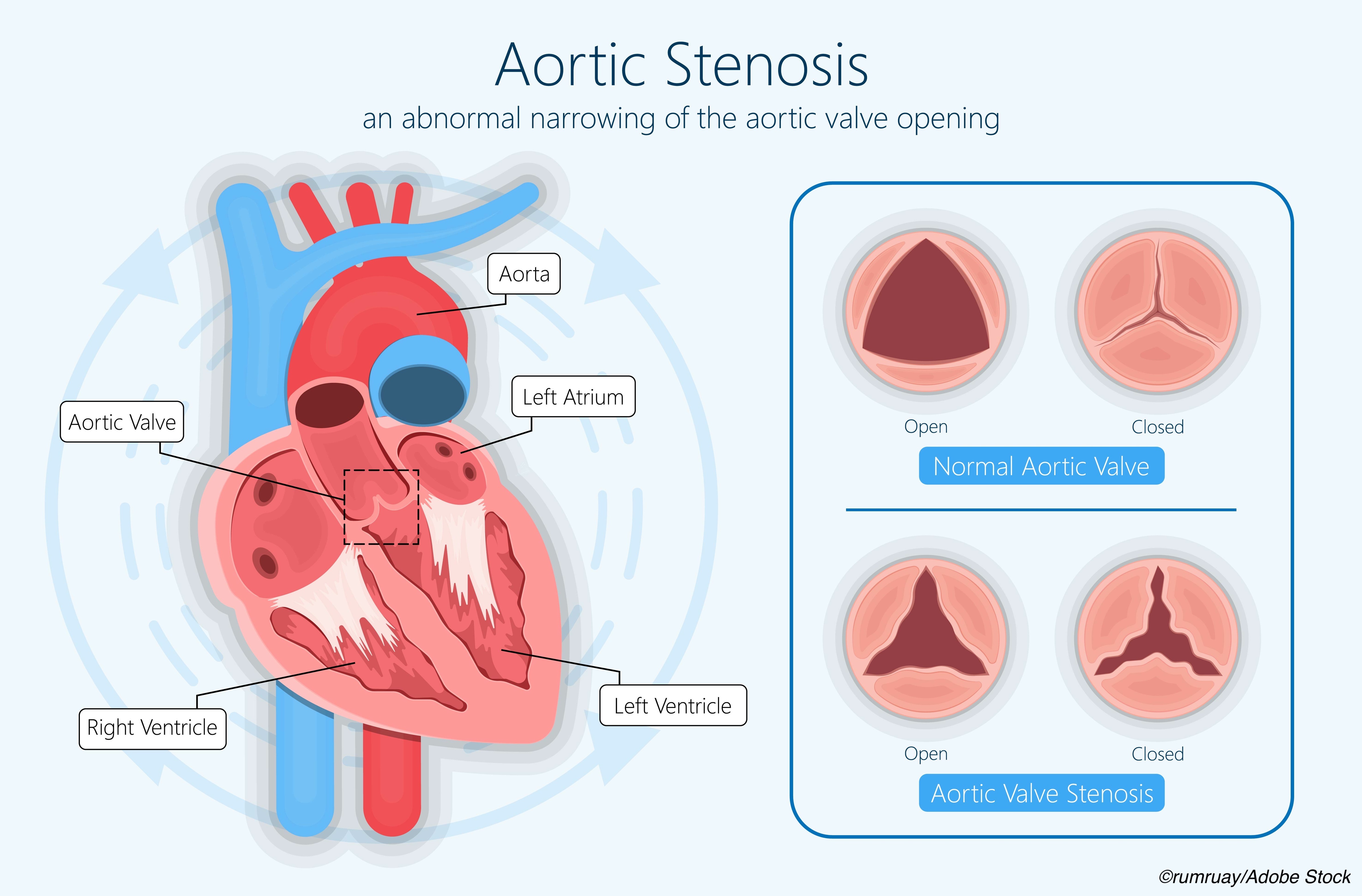
“European and North American guidelines on valvular heart disease recommend that age, surgical risk, and life expectancy be taken into consideration, together with clinical, anatomic, and procedural factors, when the Heart Team decides between surgical aortic valve replacement (SAVR) and transcatheter aortic valve implantation (TAVI) in patients with severe aortic stenosis,” wrote Andreas Martinsson, of the Sahlgrenska University Hospital, Gothenburg, Sweden, and colleagues.
“…the present study aimed to estimate survival time related to surgical risk and age after SAVR with a bioprosthesis for aortic stenosis, that is, in a population in which both SAVR and TAVI may be considered,” they explained.
To this end, Martinsson and fellow researchers included 8,353 patients ages 60 years or older (mean age: 75.1 years; 48.8% women), identified from the Swedish Cardiac Surgery Register (part of the SWEDEHEART registry), who underwent isolated SAVR with a bioprosthesis for aortic stenosis or a combination of stenosis and regurgitation. Using the EuroSCORE or EuroSCORE II, researchers risk-stratified patients preoperatively according to surgical risk into low-risk (n=7,123), intermediate-risk (n=942), or high-risk (n=288) groups.
Patients were also divided according to age and followed for a median of 5.2 years. Compared with low-risk patients, those at intermediate- and high-risk tended to be older and female and had more comorbidities.
Thirty-day mortality was 2.0% for the entire cohort, 1.2% in low-risk, 4.1% in intermediate-risk, and 8.3% in high-risk patients. In low-risk surgical patients, median survival was 10.9 years, compared with 7.3 years in intermediate-risk patients and 5.8 years in high-risk patients. Respective five-year cumulative mortality rates were 16.5%, 30.7%, and 43.0%.
In low-risk patients, median survival time was 16.2 in those ages 60-64 years and ranged to 6.1 years in those ages 85 years or older. Cumulative five-year mortality in low-risk patients ranged from 6.8% in those ages 60-64 years, to 37.7% in those 85 years or older.
Associations between age and five-year mortality risk were significant only in low-risk patients (interaction P˂0.001), with higher age at surgery significantly associated with five-year mortality (HR: 1.30 per five-year increase; 95% CI: 1.23-1.37).
Mean age at SAVR was 74.2 in men compared with 76.1 years in women (P=0.001). Men had a shorter overall median survival time compared with women (10.0 vs 10.3 years, respectively [P=0.004]). When assessed according to risk, median survival time was 10.5 years in men of low risk compared with 11.3 years in low-risk women (P=0.002).
In intermediate-risk patients, estimated median survival time was 6.6 years in men versus 7.9 years in women (P˂0.001), and 5.7 years versus 5.8 years, respectively, in high-risk men and women (P=0.10).
In an accompanying editorial, Natalie Glaser, MD, PhD, of Stockholm South General Hospital in Sweden, discussed these important findings from Martinsson and colleagues, as well as some of the study’s limitations.
“The results are interesting and add a piece to the puzzle when choosing the optimal treatment modality (SAVR or TAVR) for patients with severe aortic valve disease. The satisfactory life expectancy after SAVR has been confirmed in prior studies. The study by Martinsson et al adds the angle of surgical risk and age, where the younger patients with low surgical risk are of particular interest. Other strengths of the study include the real-world, population-based, and nationwide study design, as well as the large patient cohort with complete follow-up data,” she wrote.
Glaser highlighted the finding that in low-risk patients—but not in intermediate- or high-risk patients—age was associated with mortality.
“These results suggest that comorbidities, frailty, and anatomic and procedural factors play a more important role than chronological age in intermediate- and high-risk patients, whereas chronological age is of interest in low-risk patients. However, as the authors pointed out, the number of patients within each age category in the intermediate- and high-risk groups was limited. Furthermore, age was already included as a variable in the calculation of EuroSCORE. Therefore, these results should be interpreted with caution,” she noted, adding a cautionary note about the accuracy of the EuroSCORE versus the EuroSCORE II as well.
“In conclusion, the study by Martinsson et al conveys important information, especially in an era in which the use of TAVR is expanding to include younger and low-risk patients. It is important to recognize that the current guidelines recommend SAVR to younger and low-risk patients. The study by Martinsson et al confirms the excellent long-term survival after SAVR, especially in younger and low-risk patients. Robust evidence that long-term outcomes after TAVR are as good as those after SAVR is needed before TAVR should be recommended for these patients. Future research comparing SAVR and TAVR with follow-up for 10 years and beyond is longed for, especially in younger and low-risk patients,” concluded Glaser.
Limitations include the small sizes of both the intermediate- and high-risk populations compared with the low-risk, misclassification of risk, missing EuroSCORE values and STS scores, and the inherent risk for selection bias and residual confounding.
-
Most patients with aortic stenosis age 60 years or younger were a low surgical risk.
-
Median survival after surgical aortic valve replacement (SAVR) is more than 15 years in low-risk patients who are less than 70 years old.
Liz Meszaros, Deputy Managing Editor, BreakingMED™
This work was supported by grants from The Swedish Heart-Lung Foundation, The Swedish state under the agreement between the Swedish government and the county councils concerning economic support of research and education of doctors, and Västra Götaland Region, and Family Nils Winberg’s Foundation.
Martinnson reported no disclosures.
Glaser has received grants from the Swedish Heart-Lung Foundation and the Swedish Society of Medicine, and has a clinical postdoctoral appointment from Region, and is part of a regional agreement between Stockholm County Council and Karolinska Institutet, the Eva and Oscar Ahrén Research Foundation, and the Seraphim Hospital Foundation.
Cat ID: 308
Topic ID: 74,308,730,308,914,192,925